The most frequent asked questions for physicians
Dare to care!
Preferably Practical Questions

National boards should strive for preterm birth clinics with experienced specialist. This relates to the complex prevention of preterm birth. Although first symptoms of precocious cervical ripening may be silent, the child will be at risk for later neurodevelopmental, metabolic or cardiovascular disease. To be trained in transvaginal sonography is prerequisite to document (endo)cervical length, the utero-cervical angle or funneling. In patients with a history of anatomic malformations, cervical lesions or conization an additional speculum examination should be performed before indicating a cervical pessary. Most frequent side effects of pessaries -an increase of discharge- should be communicated. Technical training in pessary handling is useful. The clinical course may require modifications or additional treatments. It might take time to be experienced in unexpected situations because there are differences in:
- Maternal size, anatomy, parity and culture
- Pre-existing cervical shortening/thickness, opening of the internal/external cervical os
- Sensitivity to vaginal procedures (vaginismus, pain, discomfort)
- Specific obstetric situations (e.g. uterus bicornis, placenta previa etc.)
- Degree of genital prolapse or additional urinary incontinence
- Incidental or suddenly arising preterm contractions or bleeding during treatment
- Degree and kind of discharge, differential diagnosis: PPROM/ urinary incontinence
- Degree of cervical edema before removal due to contractions/pressure
It has been shown that success rates of pessary treatment increase with experience of physicians or departments by a learning curve. This also requires a basic training as demanded by the European Guideline on Prematurity. The use of medical devices is regulated by the MEDICAL DEVICE REGULATION (MDR): The manufacturer must provide instructions/ website material which is regularly modified according to post-market surveillance which must be followed. Otherwise, physicians are obliged to argue in the charts why they do not follow these instructions. Dare to care!

Explain the indication, evidence, function, and side effects (discharge) of the pessary to the patient. Place the patient in a semi-recumbent position, perform a transvaginal sonography, use centile curves of the cervical length for the indication (e.g. Salomon et al.). In risk patients it is recommended to indicate a pessary earlier (cut-off 10-25th centile) than in screening patients (cut-off 5-10th centile). Chose the size according to clinical findings and instructions:
- a) the outer lower diameter should be 65mm for nulliparous or small women and 70mm for multiparous or tall women
- b) the heights of the curvature should be 17mm rarely during the first trimester, 21mm for singleton pregnancies and smaller women, 25mm for multiple pregnancy and taller women, 30mm: rarely in women with genital prolapse
- c) the inner upper diameter should be 32mm and rarely 35mm for a wide cervix or U-shaped funneling to avoid further prostaglandin secretion.
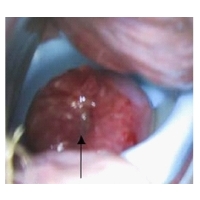
These are relative indications which can be modified for individual patients. Sizes may be changed in case of discomfort or displacement. We provide an automatic calculator for pragmatic advices on the web site: www.dr-arabin.de. A table is published in a paper: Arabin and Alfirevic, 2013, this is provided on the website as a pdf-file. Take the label of the package and stick it into the patient charts. It indicates the size and charge number. Pass the instructions to the patient and write the size and charge number on this paper in case she meets other gynecologists so that they know what was done. Fold the pessary with the smaller diameter upwards, the device should be directed towards the posterior fornix. During insertion, the pessary stays longitudinally folded until the upper vaginal fornix is reached and is then gently “pushed” as high as possible into the posterior vaginal vault with the smaller diameter around the complete cervix. The anterior rim may be gently pushed towards the sacrum. Ask the patient to get up and to indicate whether she feels comfortable. Perform only a vaginal swab if there is a high risk of PTB to inform neonatologists. Avoid inserting a pessary when contraindicated (signs of chorioamnionitis, active contractions, genital prolapse Grade III, no cervical tissue present as possibly after a previous trachelectomy). Inform the patient that in case she visits another department to provide the instructions to the physician in charge. Ask the patient for a control after one week to check the cervix and placement of the pessary. Dare to care!
In asymptomatic patients it is sufficient to examine whether the (rotated)cervix is within the upper ring. In high-risk patients (e.g. previous PTB, short cervix at insertion, clinical symptoms) an additional TVS if possible “on top of the upper cervical part” is recommended to decide whether hospital admission and/or the application of indomethacin or corticosteroids might be indicated. Pragmatically we do not recommend to apply corticosteroids if the cervical length remains >15 mm. Bed rest has not been proven to prevent PTB, just the opposite, women doing some physical exercise have lower rates of PTB. Therefore, we allow patients with a pessary to move normally but explain her to avoid physical stress (e.g. long standing). She might feel assured to move by wearing a pessary. In case of increased discharge, the differential diagnosis with PPROM is essential to avoid ascending infection and risks of neonatal infection on one side or unnecessary removal on the other side. The differential diagnosis should imply ultrasound of amniotic fluid volume and biochemical tests. When a women carries a pessary and is admitted with preterm contractions, PPROM and chorioamnionitis should be excluded, a TVS to document the cervical structure and if contractions cannot be stopped a speculum and/or clinical examination should be performed and the pessary removed to avoid cervical lesions or increased pressure in the cervical vessels/tissue. Dare to care!

A cervical pessary should routinely be removed when no risk of PTB remains, at around 37 weeks. In case that a Cesarean is scheduled it might be wise to remove the device after the patient has received an epidural before skin incision if there are no contractions or PPROM. In case of proven PPROM, the pessary should be removed. There might be exceptions such as immediately before maternal transport or in case of doubtful viability when any manipulation would risk more contractions. Nevertheless, these women must be admitted and supervised by high risk specialists. To leave a pessary should be an exception after informed consent of the patient and documentation in the charts. The removal of a pessary is shown by a you tube by Prof. Alfirevic. In general, the pessary can be removed by inserting a finger between the cervix and the upper ring. It is advisable to ensure that the cervix is pushed back through the inner ring. When there are signs of cervical edema, the woman should be informed that removal may be painful. After having removed the pessary the device can be squeezed or compressed the same way as during insertion and cautiously be removed. In case the pessary is stuck due to contractions, edema or genital prolapse, it can equally be cut by scissors usually used for episiotomies instead of removing the pessary with violence. Once the pessary is removed it should not be re-used since it is certified for single use only. Dare to care!
 Cervical discharge is the most common side effect of pessary treatment in urogynecology but also during pregnancy. The degree of discharge depends on the individual microbiome, the material and the surface of the pessaries. It is essential to inform the patient beforehand about this side effect and to re-assure her in case she is admitted to the hospital that there is no sign of PPROM. Discharge from a pessary is not equal “chorioamnionitis or infection”. Therefore, there is no indication to treat vaginal discharge by antibiotics. New studies will evaluate whether discharge can be reduced by different materials or by the additional application of probiotics. Dare to care!
Cervical discharge is the most common side effect of pessary treatment in urogynecology but also during pregnancy. The degree of discharge depends on the individual microbiome, the material and the surface of the pessaries. It is essential to inform the patient beforehand about this side effect and to re-assure her in case she is admitted to the hospital that there is no sign of PPROM. Discharge from a pessary is not equal “chorioamnionitis or infection”. Therefore, there is no indication to treat vaginal discharge by antibiotics. New studies will evaluate whether discharge can be reduced by different materials or by the additional application of probiotics. Dare to care! There is no need to perform a speculum examination in all patients before a pessary is indicated only due to cervical shortening below a certain centile. Indications for a speculum examination before pessary insertion are:
There is no need to perform a speculum examination in all patients before a pessary is indicated only due to cervical shortening below a certain centile. Indications for a speculum examination before pessary insertion are:
- History of conization or trachelectomy
- History of cervical lesions
- Suspicion of uterus duplex, possibly two cervices
- Unclear interpretation of TVS
Indications for a speculum examination during pessary insertion are:
- Discomfort, suspicion of dislocation
- Vaginal bleeding
- TVS difficult to interpret
- Suspicion of PPROM – necessity to differentiate between discharge and PPROM
These are relative indications and in case TVS can answer the clinical questions it is in the responsibility of the physician in charge to decide. Dare to care!
 In general, the indication to perform a vaginal or cervical swab is not different from other pregnant patients with an increased risk of PTB. Meanwhile, many patients have been treated with cervical pessary and physicians should inform their patients that vaginal discharge is not necessarily combined with a change of the vaginal microbiome of each individual patient. Discharge alone should not be treated with antibiotics. Antibiotics may change the microbiome more severely. In several countries. neonatologists might wish to know the pattern of the vaginal microbiome, specifically in case of streptococcus, which should be treated when delivery is threatening. However, this also holds true for other patients at risk of SPTB. A vaginal pH measurement is performed in only a few countries to diagnose a risk of bacterial vaginosis and dysbiosis. However, the sensitivity and specificity to detect PTB has never precisely been evaluated. Nevertheless, this led to unnecessary use of antibiotics with no beneficial effect. Therefore, according to the state of the art, vaginal pH measurements cannot be advised before or during pessary treatment. Dare to care!
In general, the indication to perform a vaginal or cervical swab is not different from other pregnant patients with an increased risk of PTB. Meanwhile, many patients have been treated with cervical pessary and physicians should inform their patients that vaginal discharge is not necessarily combined with a change of the vaginal microbiome of each individual patient. Discharge alone should not be treated with antibiotics. Antibiotics may change the microbiome more severely. In several countries. neonatologists might wish to know the pattern of the vaginal microbiome, specifically in case of streptococcus, which should be treated when delivery is threatening. However, this also holds true for other patients at risk of SPTB. A vaginal pH measurement is performed in only a few countries to diagnose a risk of bacterial vaginosis and dysbiosis. However, the sensitivity and specificity to detect PTB has never precisely been evaluated. Nevertheless, this led to unnecessary use of antibiotics with no beneficial effect. Therefore, according to the state of the art, vaginal pH measurements cannot be advised before or during pessary treatment. Dare to care! At the first visit, it should be checked whether the upper ring surrounds the cervix, the pessary is not dislocated and still rotated towards the sacrum, all by a cautious digital examination. In care cases, the pessary might be dislocated and can be pushed upwards as high as possible with the posterior part and then rotated by slight pressure on the anterior part. A change of the utero-cervical angle and in cervical length was demonstrated by MRI. In case of additional symptoms or in patients at increased risk of PTB, an additional TVS is useful to re-assure the patient, to indicate corticosteroids or care for an admission. In case of silent progressive shortening or funneling before 30 gestational weeks the primary choice of a pharmacological treatment should be indomethacin as 100 – 200 mg/day suppositories. Any digital examination may induce prostaglandin secretion. Therefore, it might be sufficient just to feel whether the anterior rim is still rotated during follow up. Similarly, a TVS-transducer manipulation behind the cervix can be associated with prostaglandin secretion. This can be avoided by cautiously guiding the transducer “on top” of the anterior lip of the cervix until the cervical length is visualized. In case of discharge and a suspicion of PPROM or in case of vaginal bleeding of unclear origin as well as in patients with suspected dislocation a speculum examination is indicated when early removal might be indicated or prevented. In summary: A short digital examination or an anterior TVS are combined with minimal manipulation. Dare to care!
At the first visit, it should be checked whether the upper ring surrounds the cervix, the pessary is not dislocated and still rotated towards the sacrum, all by a cautious digital examination. In care cases, the pessary might be dislocated and can be pushed upwards as high as possible with the posterior part and then rotated by slight pressure on the anterior part. A change of the utero-cervical angle and in cervical length was demonstrated by MRI. In case of additional symptoms or in patients at increased risk of PTB, an additional TVS is useful to re-assure the patient, to indicate corticosteroids or care for an admission. In case of silent progressive shortening or funneling before 30 gestational weeks the primary choice of a pharmacological treatment should be indomethacin as 100 – 200 mg/day suppositories. Any digital examination may induce prostaglandin secretion. Therefore, it might be sufficient just to feel whether the anterior rim is still rotated during follow up. Similarly, a TVS-transducer manipulation behind the cervix can be associated with prostaglandin secretion. This can be avoided by cautiously guiding the transducer “on top” of the anterior lip of the cervix until the cervical length is visualized. In case of discharge and a suspicion of PPROM or in case of vaginal bleeding of unclear origin as well as in patients with suspected dislocation a speculum examination is indicated when early removal might be indicated or prevented. In summary: A short digital examination or an anterior TVS are combined with minimal manipulation. Dare to care! Every specialist should take time to explain clinical and sonographic findings and options for therapy including the most recent results. The wy of communication will have an impact whether a patient accepts or declines to accept a pessary. In very few large multiparous patients the pessary may be too small to stay in place and may dislocate. In these patients, we might adapt a customized larger pessary (produced by special modelling) or use the largest size. In patients with vaginism, it might be complicated to insert and remove the pessary due to muscular tension. Around 1/100 patients may complain to feel uncomfortable with a pessary. This can even indicate a removal of the pessary or possibly to try a smaller size, which may help that the device is tolerated. Dare to care!
Every specialist should take time to explain clinical and sonographic findings and options for therapy including the most recent results. The wy of communication will have an impact whether a patient accepts or declines to accept a pessary. In very few large multiparous patients the pessary may be too small to stay in place and may dislocate. In these patients, we might adapt a customized larger pessary (produced by special modelling) or use the largest size. In patients with vaginism, it might be complicated to insert and remove the pessary due to muscular tension. Around 1/100 patients may complain to feel uncomfortable with a pessary. This can even indicate a removal of the pessary or possibly to try a smaller size, which may help that the device is tolerated. Dare to care! Years ago, we evaluated whether disinfectants prevent bacterial colonization of pessaries. Since solutions and recommendations for disinfectants varies in different countries, our notified body advised NOT to recommend disinfection since not all solutions can be evaluated in terms of hygiene or changes of the material. Therefore, we do not recommend the use of disinfections before insertion any longer. The devices are tempered after production and examined by bioburden tests at regular intervals. PHYSICIANS SHOULD NOT USE THE PESSARY FOR A SECOND TIME IN ANOTHER PATIENT. If they might wish to show pessaries to their patients, physical washing might be enough to clean a pessary. Normally, the material also withstands sterilization – however, it is declared as a product for single use to avoid contamination. We provide distributors with “proof pessaries”. Dare to care!
Years ago, we evaluated whether disinfectants prevent bacterial colonization of pessaries. Since solutions and recommendations for disinfectants varies in different countries, our notified body advised NOT to recommend disinfection since not all solutions can be evaluated in terms of hygiene or changes of the material. Therefore, we do not recommend the use of disinfections before insertion any longer. The devices are tempered after production and examined by bioburden tests at regular intervals. PHYSICIANS SHOULD NOT USE THE PESSARY FOR A SECOND TIME IN ANOTHER PATIENT. If they might wish to show pessaries to their patients, physical washing might be enough to clean a pessary. Normally, the material also withstands sterilization – however, it is declared as a product for single use to avoid contamination. We provide distributors with “proof pessaries”. Dare to care!Preferably Theoretical Questions
 Any clinical procedures should be performed under supervision of experienced clinicians. Even the communication with patients needs experience. Although statisticians try to pretend that everything can be predicted this is not true. We live in a world of uncertainty where we also have to make fast decisions not only based on theory bit also experience. Worldwide, there are different guidelines about prevention of sPTB . The WHO underlines that screening for a disease is only recommended when the outcome can be improved. Unfortunately, after the first publication of a RCT in singleton and twin pregnancies by Goya et al. 2012 and of the sub-analysis of Liem et al. 2013 several studies were performed by unexperienced staff which might have had an impact on negative results. In several retrospective meta-analyses low-quality trials are used. The authors rarely follow the study pyramid (Figure 1). Results from these meta-analyses can be controversial when applying different selection criteria for included RCTs. Underpowered and unregistered RCTs should not be considered for any meta-analysis. It seems wise to wait for results from a running prospective meta-analysis. It cannot be expected that pessaries can prevent PTB in all patients. It has been suggested that in patients with a history of PPROM the pessary may be less effective. More studies are needed to explain the effect of pessaries in the cervico-vaginal space where the tissue is sensitive to dysbiosis. Mainly in twin pregnancies studies show benefits. Long term outcome after 3 years in children after pessary treatment demonstrate a number to treat (NTT) to prevent severe handicap or death of 1/6. In general, pessary treatment should follow the Triple Aim to increase patient satisfaction, health outcomes in a population and to reduce costs (Figure 2). Dare to care!
Any clinical procedures should be performed under supervision of experienced clinicians. Even the communication with patients needs experience. Although statisticians try to pretend that everything can be predicted this is not true. We live in a world of uncertainty where we also have to make fast decisions not only based on theory bit also experience. Worldwide, there are different guidelines about prevention of sPTB . The WHO underlines that screening for a disease is only recommended when the outcome can be improved. Unfortunately, after the first publication of a RCT in singleton and twin pregnancies by Goya et al. 2012 and of the sub-analysis of Liem et al. 2013 several studies were performed by unexperienced staff which might have had an impact on negative results. In several retrospective meta-analyses low-quality trials are used. The authors rarely follow the study pyramid (Figure 1). Results from these meta-analyses can be controversial when applying different selection criteria for included RCTs. Underpowered and unregistered RCTs should not be considered for any meta-analysis. It seems wise to wait for results from a running prospective meta-analysis. It cannot be expected that pessaries can prevent PTB in all patients. It has been suggested that in patients with a history of PPROM the pessary may be less effective. More studies are needed to explain the effect of pessaries in the cervico-vaginal space where the tissue is sensitive to dysbiosis. Mainly in twin pregnancies studies show benefits. Long term outcome after 3 years in children after pessary treatment demonstrate a number to treat (NTT) to prevent severe handicap or death of 1/6. In general, pessary treatment should follow the Triple Aim to increase patient satisfaction, health outcomes in a population and to reduce costs (Figure 2). Dare to care! Both treatments seem to be indicated in a similar group of patients with singleton pregnancies and cervical shortening. At the present stage, there are different options in case of cervical shortening to start with or even to combine both treatments. In twin pregnancies, there is no evidence that vaginal progesterone reduces sPTB (Dodd et al. 2017). Therefore, pessaries maybe preferred. This is supported by the first RCT comparing both treatments in twin pregnancies: In a predefined subgroup a cervical pessary was significantly more effective in reducing poor outcome and SPTB rates (Dang et al, 2019). One RCT randomizing patients with singleton pregnancies for vaginal progesterone, could show that the additional application of a pessary could improve the neonatal outcome by reducing PTB rates (Saccone et al. 2017). It is recommend to start any treatment earlier in pateints with additional risks as compared to screening patients. By adding vaginal progesterone to a pessary no significant impact besides a shortened stay on the NICU was found in a historic cohort (Stricker et al. 2016). More good studies are needed to compare the treatments and to select specific options. Dare to care!
Both treatments seem to be indicated in a similar group of patients with singleton pregnancies and cervical shortening. At the present stage, there are different options in case of cervical shortening to start with or even to combine both treatments. In twin pregnancies, there is no evidence that vaginal progesterone reduces sPTB (Dodd et al. 2017). Therefore, pessaries maybe preferred. This is supported by the first RCT comparing both treatments in twin pregnancies: In a predefined subgroup a cervical pessary was significantly more effective in reducing poor outcome and SPTB rates (Dang et al, 2019). One RCT randomizing patients with singleton pregnancies for vaginal progesterone, could show that the additional application of a pessary could improve the neonatal outcome by reducing PTB rates (Saccone et al. 2017). It is recommend to start any treatment earlier in pateints with additional risks as compared to screening patients. By adding vaginal progesterone to a pessary no significant impact besides a shortened stay on the NICU was found in a historic cohort (Stricker et al. 2016). More good studies are needed to compare the treatments and to select specific options. Dare to care! The first patient why a pessary was placed indicated by TVS was a woman who had already lost two children due to preterm birth and received a cerclage in her third (twin) pregnancy, but presented with funneling to the stich at 17 weeks. A pessary was placed on top of this cervix and pregnancy was prolonged to 37 weeks. This was an individual emergency situation. There are up to now no randomized trials (RCT) but observational case series suggesting better outcomes when a patient with a cerclage additionally received a pessary. RCTs to compare both treatment options in singleton and twin pregnancies or even combinations are still ongoing. Dare to care!
The first patient why a pessary was placed indicated by TVS was a woman who had already lost two children due to preterm birth and received a cerclage in her third (twin) pregnancy, but presented with funneling to the stich at 17 weeks. A pessary was placed on top of this cervix and pregnancy was prolonged to 37 weeks. This was an individual emergency situation. There are up to now no randomized trials (RCT) but observational case series suggesting better outcomes when a patient with a cerclage additionally received a pessary. RCTs to compare both treatment options in singleton and twin pregnancies or even combinations are still ongoing. Dare to care! Intramuscular progesterone was indicated in patients with a history of preterm birth without cervical shortening (yet) mainly in Angloamerican countries. The medication is rarely used in central Europe. The more recent PROLONG study suggests that i.m. progesterone has no beneficial effect. In Germany, 17alpha OH-progesterone Caproate (Proluton®) is not any longer available. There are no systematic studies showing that patients who already have 17alphaOH-progesterone may benefit from an additional pessary – but at least the patient can be re-assured that the pessary does no harm – since individual patients have been treated with both. Dare to care!
Intramuscular progesterone was indicated in patients with a history of preterm birth without cervical shortening (yet) mainly in Angloamerican countries. The medication is rarely used in central Europe. The more recent PROLONG study suggests that i.m. progesterone has no beneficial effect. In Germany, 17alpha OH-progesterone Caproate (Proluton®) is not any longer available. There are no systematic studies showing that patients who already have 17alphaOH-progesterone may benefit from an additional pessary – but at least the patient can be re-assured that the pessary does no harm – since individual patients have been treated with both. Dare to care! The management should be dependent on additional clinical symptoms, the magnitude of cervical dilatation and the gestational age. Signs of chorioamnionitis and contractions should be excluded at admission. Transvaginal scans should assess the degree of funnelling, sludge, and cervical length. Before 24 weeks, obstetricians might consider cervical cerclage in singleton pregnancies. We would prefer to place or leave a pessary in place to avoid risks in case of hidden chorioamnionitis. The patient may be placed in Trendelenburg position, indomethacin (supp.) can be indicated before 32 weeks to reduce prostaglandin secretion. Dependent on the width of funnelling an upper diameter of 32mm in case of V-shaped funnelling and of 35mm in case of U-shaped funnelling should be selected. Corticosteroids or tocolytics may be indicated. A swab may be performed due to the risk of preterm birth- to inform neonatologists or to start antibiotics in case of streptococcus or resistant germs. A first still unpublished observational study in patients with funnelling showed that pessary alone is not connected with increased risks of neonatal infections. Dare to care!
The management should be dependent on additional clinical symptoms, the magnitude of cervical dilatation and the gestational age. Signs of chorioamnionitis and contractions should be excluded at admission. Transvaginal scans should assess the degree of funnelling, sludge, and cervical length. Before 24 weeks, obstetricians might consider cervical cerclage in singleton pregnancies. We would prefer to place or leave a pessary in place to avoid risks in case of hidden chorioamnionitis. The patient may be placed in Trendelenburg position, indomethacin (supp.) can be indicated before 32 weeks to reduce prostaglandin secretion. Dependent on the width of funnelling an upper diameter of 32mm in case of V-shaped funnelling and of 35mm in case of U-shaped funnelling should be selected. Corticosteroids or tocolytics may be indicated. A swab may be performed due to the risk of preterm birth- to inform neonatologists or to start antibiotics in case of streptococcus or resistant germs. A first still unpublished observational study in patients with funnelling showed that pessary alone is not connected with increased risks of neonatal infections. Dare to care! In patients with intact membranes, we would advise to only perform a swab in case of threatening preterm birth to communicate the results to neonatologists and to exclude streptococcus. Even when swabs are performed, pessaries can be placed without delay, e.g. without waiting for the result. The use of antibiotics changes the vaginal microbiome and may result in a disbalanced pattern of benign or pathologic variants of lactobacillus. It has been proven in animals, that some bacteria can directly change the structure of the cervical tissue. Within the study of Goya et al. (2012), the type of colonization remained the same during pessary use. Within some studies a high number of patients were treated with antibiotics, which might have even increased the risk for preterm birth or cerebral palsy. Chronic infection of the decidua or membranes (increased risk after curettage or ART) does not correspond with the vaginal microbiome. Dare to care!
In patients with intact membranes, we would advise to only perform a swab in case of threatening preterm birth to communicate the results to neonatologists and to exclude streptococcus. Even when swabs are performed, pessaries can be placed without delay, e.g. without waiting for the result. The use of antibiotics changes the vaginal microbiome and may result in a disbalanced pattern of benign or pathologic variants of lactobacillus. It has been proven in animals, that some bacteria can directly change the structure of the cervical tissue. Within the study of Goya et al. (2012), the type of colonization remained the same during pessary use. Within some studies a high number of patients were treated with antibiotics, which might have even increased the risk for preterm birth or cerebral palsy. Chronic infection of the decidua or membranes (increased risk after curettage or ART) does not correspond with the vaginal microbiome. Dare to care! In twin pregnancies: Never, see meta-analysis of Dodd et al. The meta-analysis of Romero with a positive result for vaginal progesterone was only due to one trial from Egypt which was neither placebo-controlled nor pre-registered. According to Prior these trials should not be included in meta-analyses (Prior et al.2017). A first direct comparison of pessary and vaginal progesterone showed advantages of the pessary (Dong et al. 2019). In singleton pregnancies: Pessary treatment was our first choice in patients with cervical shortening up to 2011. After the publication of Hassan et al. we performed a historic cohort study in singleton pregnancies and added vaginal progesterone both in screening and risk patients, but did not find differences apart from a stay on NICU which might have been due to the historic model (Stricker et al. 2016 ). A first direct comparison did not show significant differences between vaginal progesterone and pessary (Cruz-Melguizo et al. 2018) in singleton pregnancies to prevent preterm birth. More studies are needed to clarify the effect of different interventions or their combined use. Dare to care!
In twin pregnancies: Never, see meta-analysis of Dodd et al. The meta-analysis of Romero with a positive result for vaginal progesterone was only due to one trial from Egypt which was neither placebo-controlled nor pre-registered. According to Prior these trials should not be included in meta-analyses (Prior et al.2017). A first direct comparison of pessary and vaginal progesterone showed advantages of the pessary (Dong et al. 2019). In singleton pregnancies: Pessary treatment was our first choice in patients with cervical shortening up to 2011. After the publication of Hassan et al. we performed a historic cohort study in singleton pregnancies and added vaginal progesterone both in screening and risk patients, but did not find differences apart from a stay on NICU which might have been due to the historic model (Stricker et al. 2016 ). A first direct comparison did not show significant differences between vaginal progesterone and pessary (Cruz-Melguizo et al. 2018) in singleton pregnancies to prevent preterm birth. More studies are needed to clarify the effect of different interventions or their combined use. Dare to care!
 We do not recommend to remove a pessary to place a cerclage in patients with progressive shortening since we are afraid of amnioinfection and sepsis. It may be wise to additionally treat these patients with indomethacin supp, at least 200 mg/day before 32 weeks, to admit the patient, let her be placed in Trendelenburg and due close surveillance to exclude chorioamnionitis. It is hard to predict in which patients prolongations should be strived for. When patients have previous PPROM, several curettages or ART, chronic inflammation may be more frequently present impairing the pessary effect. Dare to care!
We do not recommend to remove a pessary to place a cerclage in patients with progressive shortening since we are afraid of amnioinfection and sepsis. It may be wise to additionally treat these patients with indomethacin supp, at least 200 mg/day before 32 weeks, to admit the patient, let her be placed in Trendelenburg and due close surveillance to exclude chorioamnionitis. It is hard to predict in which patients prolongations should be strived for. When patients have previous PPROM, several curettages or ART, chronic inflammation may be more frequently present impairing the pessary effect. Dare to care! Overdistension as described for twin pregnancies is even more pronounced in triplet pregnancies. Therefore, cervical shortening occurs earlier leading to higher PTB rates of triplets as compared to twins. Up to now, there are no larger trials including triplet pregnancies only. In an unpublished historic cohort in the Netherlands we could show a prolongation of pregnancies in patients with triplets, early transvaginal sonography and early pessary treatment as compared to controls without that treatment. Dare to care!
Overdistension as described for twin pregnancies is even more pronounced in triplet pregnancies. Therefore, cervical shortening occurs earlier leading to higher PTB rates of triplets as compared to twins. Up to now, there are no larger trials including triplet pregnancies only. In an unpublished historic cohort in the Netherlands we could show a prolongation of pregnancies in patients with triplets, early transvaginal sonography and early pessary treatment as compared to controls without that treatment. Dare to care! Patients with placenta previa may start bleeding with cervical shortening due to a shift of layers in the lower uterine segment. Theoretically, a stabilization of the cervix may prevent cervical shortening and vaginal bleeding. The simultaneous use of pessaries with vaginal progesterone resulted in a 2.5-fold decrease in the rate of vaginal dysbiosis, bleeding and preterm birth (Barinov et al. 2016). Unfortunately, we only suspect that the effect was due to a pessary. Placenta previa is no contraindication for a pessary. Whether a pessary should be applied early in gestational even when the cervix is not shortened or whether it should be only indicated in case of precocious ripening as determined by TVS requires more research. Dare to care!
Patients with placenta previa may start bleeding with cervical shortening due to a shift of layers in the lower uterine segment. Theoretically, a stabilization of the cervix may prevent cervical shortening and vaginal bleeding. The simultaneous use of pessaries with vaginal progesterone resulted in a 2.5-fold decrease in the rate of vaginal dysbiosis, bleeding and preterm birth (Barinov et al. 2016). Unfortunately, we only suspect that the effect was due to a pessary. Placenta previa is no contraindication for a pessary. Whether a pessary should be applied early in gestational even when the cervix is not shortened or whether it should be only indicated in case of precocious ripening as determined by TVS requires more research. Dare to care!